
Frances Taylor-Brown
EBVS® European Specialist in Veterinary Neurology and RCVS Specialist in Veterinary Neurology
BSc(Hons) BVetMed(Hons) MVetMed DipECVN MRCVS
What is acquired myasthenia gravis?
Acquired myasthenia gravis (aMG) is an immune-mediated condition which occurs as a result of autoantibodies usually directed against the acetylcholine receptors which are found at the nerve-muscle junction.
What is the typical signalment of presenting cases?
It is more common in large breed dogs and has a bimodal presentation affecting dogs either 4 months to 4 years or 9 to 13 years of age.
How do dogs with acquired myasthenia gravis present?
Dogs with aMG can present in one of three ways:
- The most common presentation is generalised, accounting for 60% of cases. These patients commonly present with exercise-induced weakness, megaoesophagus (leading to regurgitation), dysphagia and facial nerve paresis (causing a bilateral decreased palpebral reflex).
- Acquired myasthenia gravis can also be a focal presentation where there is weakness of an isolated muscle group and this accounts for about 35% of cases. Commonly affected muscles include the oesophagus (leading to megaoesophagus), pharyngeal/laryngeal muscles (leading to dysphagia and/or loss of bark) or facial muscles (leading to a decreased palpebral reflex).
- The least common presentation is the fulminating form which accounts for the remaining 5% of cases. These patients present with an acute and rapidly progressive non-ambulatory tetraparesis with decreased muscle tone and decreased spinal reflexes. These patients often have facial nerve weakness and decreased gag reflex.
How is acquired myasthenia gravis diagnosed?
The gold standard test for diagnosing aMG is ACh receptor autoantibody test. Unfortunately, it is possible to get a false negative result in 2% of generalised cases and this is referred to as seronegative.
Possible reasons for seronegative acquired myasthenia gravis:
- Pre-treatment with immunosuppressive treatment
- Most autoantibodies bound to skeletal muscle and therefore not detectable
- Damage to the antigenic epitopes during solubilization therefore not able to detect autoantibodies
- Autoantibodies directed against other components of the postsynaptic neuromuscular junction
In dogs that have a negative result it is worth repeating the test 1 to 2 months later as some patients can be seronegative during the early course of the disease and subsequently seroconvert.
What other tests can be performed whilst pending the results of the ACh receptor autoantibody test?
Supplementary testing is useful whilst pending ACh receptor autoantibody test results in order to help increase the index of suspicion of the diagnosis of aMG however these other tests lack sensitivity and specificity.
- Thoracic radiographs or CT scan of thorax are useful to evaluate for presence of megaoesophagus which is very common in dogs with aMG and is present in 85% of cases. Thoracic imaging also allows evaluation for co-existing pathology, particularly a cranial mediastinal mass (usually a thymoma) which is present in 3% of dogs with aMG, more common in generalised or fulminant presentations.
 Thoracic radiograph showing megaoesophagus
Thoracic radiograph showing megaoesophagus 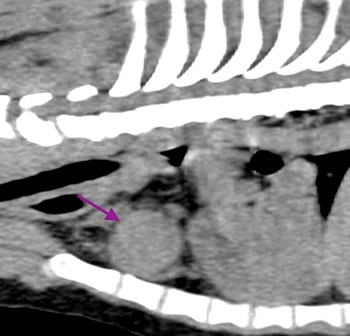 Thorax CT scan showing cranial mediastinal mass
Thorax CT scan showing cranial mediastinal mass
- Additional investigations to evaluate for concomitant disease includes haematology, biochemistry, urinalysis and abdominal imaging.
- Pharmacological testing can be performed with acetylcholinesterase inhibitors (edrophonium or neostigmine), however, it is possible to get false positive responses in dogs with exercise-induced weakness as a result of myopathic or neuropathic diseases, and in dogs with focal or fulminant presentations, it is likely to see false negative responses.
- Electrodiagnostic studies can also be performed with particular focus on repetitive nerve stimulation where in generalised and fulminant cases noting a >10% decrement in the amplitude of the compound muscle action potential provides a presumptive diagnosis of aMG.
What treatment should be considered?
Treatment can be divided into three components:
- Supportive care is really important for managing dogs with aMG as megaoesophagus and associated aspiration pneumonia is the most common cause of death.
- Symptomatic treatment is recommended with anticholinesterase inhibitor therapy (pyridostigmine) dosed to effect. Initiating treatment with pyridostigmine should be performed in hospital as there can be adverse side effects due to a cholinergic crisis.
- In those patients that fail to respond to symptomatic treatment then it is possible to consider initiating immunomodulatory therapy such as prednisolone, however, this can also be complicated due to adverse effects such as exacerbation of skeletal muscle weakness and compromised immune function in the presence of aspiration pneumonia.

What is the prognosis for dogs with acquired myasthenia gravis?
Overall prognosis is guarded due to frequent presence of megaoesophagus and risk of aspiration pneumonia. The one-year mortality rate is reported to be 50%. However spontaneous remission is common and it has been reported that up to 89% of dogs treated with anticholinesterase inhibitor therapy alone went into remission within an average of six months following diagnosis.
Top Tips
- Acquired myasthenia gravis is a relatively common diagnosis and can present in a number of ways
- If aMG is a differential diagnosis, test for autoantibodies against the ACh receptor prior to initiating treatment with immunosuppressive drugs
- Supportive care to manage megaoesophagus and prevent aspiration pneumonia is important to improve prognosis
For more information or to speak to one of our Neurologists in Somerset please call 01823 653510.
