
Canine cognitive dysfunction
Simon Bertram
RCVS recognised Specialist in Veterinary Neurology
EBVS® European Specialist in Veterinary Neurology
DVM MVetMed DipECVN MRCVS
What is canine cognitive dysfunction (CCD)?
CCD is also referred to as ‘canine dementia’ and is a neurobehavioural syndrome identified in older dogs (generally those >8 years). It shares similarities with human Alzheimer’s with deposition of amyloid plaques and cerebral amyloid angiopathy throughout the brain. The prevalence increases with age with 28% of dogs aged 11-12 years showing clinical signs, and up to 68% of dogs aged 15-16 years showing clinical signs. The condition is poorly recognised by owners and vets with only 2% of potential cases being diagnosed. It's a progressive condition and cannot be cured, but management strategies like medication, dietary supplements, and environmental enrichment can help alleviate symptoms and improve quality of life for affected dogs.
What are the main risk factors?
The major risk factor for CCD is age. However other risk factors identified include genetics, nutrition (dogs fed a low grade commercial diet or non-commercial diets were at higher risk of developing CCD), training history and concurrent diseases (particularly idiopathic epilepsy but there also is a possible association with hypothyroidism and hypertension).
What are the main clinical signs?
The main clinical signs associated with CCD include:
- Disorientation: Confusion or getting lost in familiar surroundings.
- Changes in sleep patterns: Increased restlessness at night or sleeping more during the day.
- Decreased activity levels: Reduced interest in playing or going for walks.
- Loss of house training: Accidents indoors despite previous house training.
- Alterations in social interactions: Changes in how the dog interacts with family members or other pets.
- Anxiety or agitation: Restlessness, pacing, or vocalizing for no apparent reason.
- Decreased responsiveness: Slower response to commands or cues.
- Changes in appetite or drinking habits: Increased or decreased appetite and/or thirst.
- Repetitive behaviours: Engaging in repetitive actions like pacing or licking.
- Loss of learned behaviours: Forgetting previously learned commands or tricks.
How is CCD diagnosed?
Canine cognitive dysfunction (CCD) is typically diagnosed through a combination of clinical signs reported by the owner, physical examination by a neurologist to rule out other medical conditions with similar symptoms, and sometimes specific cognitive function tests. There isn't a definitive diagnostic test for CCD, so diagnosis often involves ruling out other possible causes of the observed symptoms. Blood tests, urine tests, and imaging studies may be conducted to rule out underlying medical conditions. Sometimes MRI will be performed to rule out other conditions of the brain (esp. brain tumours) and look for changes typical for CCD (see below).
If other conditions are ruled out and the clinical signs are consistent with CCD, a diagnosis may be made based on the dog's age and symptom presentation.
Cognitive function tests:
CCDR, CADES, and DISHAA are all acronyms related to tools or methods used in the assessment or diagnosis of cognitive dysfunction in dogs:
- CCDR: Canine Cognitive Dysfunction Rating (CCDR) is a rating scale used by veterinarians to assess the severity of cognitive dysfunction in dogs. It evaluates various aspects of the dog's behaviour and cognitive function to determine the level of impairment.
- CADES: Canine Dementia Scale (CADES) is another rating scale used to assess cognitive dysfunction in dogs. Similar to CCDR, CADES evaluates different aspects of the dog's behaviour and cognitive abilities to gauge the severity of cognitive impairment.
- DISHAA: DISHAA stands for Dog Impairment in Spontaneous Home Activities Assessment. It is a method developed to assess cognitive dysfunction in dogs based on their spontaneous activities at home. This method involves observing the dog's behaviour and interactions in its natural environment to detect signs of cognitive decline.
Typical findings on MRI
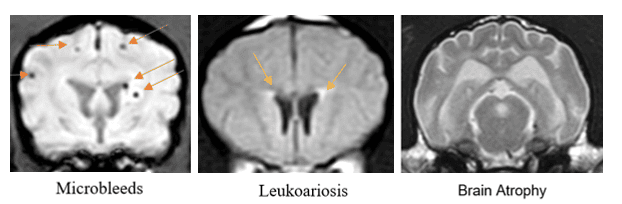
Typical findings on MRI (Magnetic Resonance Imaging) related to canine cognitive dysfunction (CCD) are not always specific, but they may show changes consistent with brain atrophy and other age-related changes. These changes can include:
- Cerebral Atrophy: Shrinkage of the brain tissue, particularly in regions associated with memory and cognition.
- Ventricular Enlargement: Expansion of the fluid-filled spaces within the brain (ventricles), which can occur due to brain tissue loss.
- White Matter Lesions: Abnormalities in specific areas of the white matter of the brain, which is called Leukoariosis
- Microbleeds: very small areas of old and new bleed in the brain has been shown to be associated with CCD
- Size of the interthalamic adhesion: this is an area of the midbrain where the left and the right side of the brain meet. It has been shown that a reduction if the size of this structure is associated with CCD.
These findings on MRI can provide supportive evidence for a diagnosis of cognitive dysfunction in dogs, especially when correlated with clinical signs. However, it's important to note that these changes are not unique to CCD and can also be seen in other neurological conditions or as part of the normal aging process.
Is there any treatment?
The treatment and management of canine cognitive dysfunction (CCD) typically involve a combination of strategies aimed at slowing the progression of cognitive decline and improving the quality of life for affected dogs. Some common approaches include:
- Nutrition: Hills B/D is high in anti-oxidants and reported to improve brain function
- Medium chain triglycerides (MCT) oils: provide an alternative energy source for the brain
- Supplements: Phospatidylserine + S-Adenosyl-L-methionine (SAMe)
- Environmental enrichment: regular exercise, social interactions and introduction of new toys and games has been shown to prevent or delay cognitive decline in older dogs
- Regular Exercise: Physical activity is important for maintaining overall health and cognitive function in dogs. Regular walks, playtime, and other forms of exercise can help reduce anxiety, improve mood, and promote mental stimulation.
- Routine and Structure: Establishing a predictable daily routine and environment can help reduce confusion and anxiety in dogs with CCD.
- Behavioural Therapy: Working with a veterinary behaviourist to address specific behavioural issues associated with CCD, such as house soiling or night-time restlessness, can be helpful.
- Anti-anxiety medications: gabapentin/pregabalin, fluoxetine, benzodiazepines
- Selegiline: thought to exert beneficial effects by restoring dopaminergic balance some benefit has been shown in clinical trials but this will vary markedly according to the individual dog and the duration of use
- Other complementary therapies: with the primary goal of reducing anxiety and normalising the sleep/wake cycle include melatonin, acupuncture, pheromones (DAP), lavender essential oils, valerian root. There is no evidence to support the use of these therapies.
While there is no cure for CCD, these management strategies can help slow the progression of the disease and improve the dog's quality of life. It's essential for owners to work closely with their veterinarian to develop a comprehensive treatment plan tailored to the individual needs of their dog.
Top Tips:
- The diagnosis is based on specific clinical signs and the combination of any other intracranial structural disease
- Owner questionnaires like DISHAA, CCDR and CADES are very useful
- “Typical” MRI changes are not always present
- Despite there not being any treatment different management strategies can help to improve or slow down the deterioration of Quality of life
For more information or to speak to one of our Neurologists please call 01823 653510 or email This email address is being protected from spambots. You need JavaScript enabled to view it. .
Neuromuscular disease
What is the neuromuscular system?
The neuromuscular system is the nervous system outside of the brain and spinal cord, and includes the nerves and muscles (and their junction). The nerves of the neuromuscular system include both the nerves that of the head (cranial nerves) and nerves leaving the spinal cord that control the muscles of the limbs. The junction between the nerve and the muscle is called the neuromuscular junction.
The neuromuscular system is important for motor activity (walking, standing, chewing food, swallowing). Signals travel along a nerve as an electrical current, which then must travel across the gap (neuromuscular junction) to reach the muscle.
What signs are associated with a neuromuscular disease?
Dogs or cats that present with neuromuscular disease commonly present with varying degrees of weakness, and possible muscle wastage. This weakness can affect any muscle in the body and may cause animals to be unable to exercise normally, or even affect their swallowing and may cause regurgitation.
This weakness may be related to disease in the nerve (neuropathy), the neuromuscular junction (junctionopathy) or the muscle itself (myopathy). In mild cases the weakness may only be intermittent and associated by exercise, in more severe cases the animal may be unable to support its own weight, unable to hold its head up and have breathing difficulty.
What diseases can cause neuromuscular signs?
There are a large number of diseases that can cause neuromuscular signs. These can be directly associated with the nerve, neuromuscular junction or myopathy; or a disease elsewhere in the body that is having an effect on the function of the neuromuscular system.
Diseases that can cause a neuropathy, junctionopathy or myopathy may include:
- Infectious diseases (e.g. neosporosis, toxoplasmosis, tetanus, botulism)
- Immune mediated diseases (inflammation of the nerve – neuritis or polyradiculoneuritis, destruction of acetylcholine receptor – myasthenia gravis; inflammation of the muscle – myositis)
- Toxins
- Inherited and degenerative diseases
Diseases that may cause an indirect effect on the neuromuscular system:
- Endocrine disease: hypothyroidism, diabetes, hyperadrenocorticism, hypoadrenocorticism
- Cancer
- Kidney` disease
- Heart and lung disease
How do we diagnose neuromuscular disease?
The first step to diagnosing neuromuscular disease is to rule out the diseases that may cause an indirect effect on the neuromuscular system. Tests that may be performed include:
- Blood profile (including tests for hormonal and infectious diseases or specific tests if we are concerned about Myasthenia Gravis)
- Imaging (such as an X-ray, ultrasound or CT scan) of the thorax and abdomen
- Electrodiagnostics - this is where a small electrical current is delivered to an individual nerve or muscle and we can evaluate the muscle response to this stimulation.
- Biopsy of the neve or muscle to try and identify whether there is inflammation or degeneration of the nerve or muscle.
What is the treatment for neuromuscular disease?
The treatment for neuromuscular disease can be varied and depends on the suspected underlying cause. It is important to be aware that even if the underlying cause is treatable, many may take weeks to improve.
What is the prognosis?
The prognosis for neuromuscular disease, much like the treatment, is variable and depends on the underlying cause. Some conditions such as neuromuscular disease caused by cancer, an inherited neuropathy or myopathy may be associated with a poor prognosis. However, many conditions may have a good prognosis with appropriate treatment.
Myasthenia gravis
What is Myasthenia gravis and what are the causes?
Myasthenia gravis is a disease causing muscle weakness. It affects the area where nerves meet the muscles called the neuromuscular junction. Normally, nerve signals are passed on to the muscle with the help of small molecules (a chemical messenger called acetylcholine) crossing this junction and docking onto a specific receptor (acetylcholine receptor). This will trigger the contraction of the muscle. In Myasthenia Gravis there is abnormal transmission of the message between the nerves and the muscles which causes weakness.
Congenital Myasthenia gravis:animals born with myasthenia gravis are born with too few acetylcholine receptors and this disturbs the normal function of the neuromuscular junction. This has been described in Jack Russell terriers, Springer Spaniels and Smooth-haired Fox terriers.
Acquired Myasthenia gravis: this is the more common form of the disease and is considered to be an autoimmune disease. The body’s immune system attacks and destroys the acetylcholine receptors. It is not known why the immune system suddenly decides to attack these receptors in some dogs. Rarely Myasthenia Gravis can be triggered by cancer, or can be associated with other immune diseases affecting the nerves or muscles, or be related to an under-active thyroid gland. It is seen most commonly in Akita Inus, Terrier breeds, German Shorthaired Pointers, German Shepherd dogs and Golden retrievers, Abyssinians and Somali cats.
What are the signs of Myasthenia gravis?
Depending on which muscles of the body will be affected the clinical signs can vary from exercise intolerance (the animal seems normal for the first seconds or minutes and progressively gets weaker and will need to sit down being unable to get up for a couple of seconds to minutes), to complete inability to stand or walk to inability to swallow or keep food down (due to a problem with the food pipe).
How is Myasthenia gravis diagnosed?
The investigations vary depending on the subtype of Myasthenia gravis. In most cases the best test to diagnose acquired MG in is a blood test which looks for antibodies directed toward the acetylcholine receptor. Sometimes another test needs to be performed where a drug is given which quickly (but only shortly) reverses the weakness if it is caused by MG. Electrodiagnostic studies can be very useful in ruling out other neuromuscular diseases that might cause similar signs. In cases were a congenital form is suspected a muscle biopsy needs to be taken and sent away for analysis. If there is a suspicion that the MG was triggered by an underlying disease, like cancer, then other investigations may be required: chest X-Rays, abdominal ultrasound or a CT scan.
What treatment options are available?
Specific treatment tries to diminish the clinical signs by giving a medication to help with the transmission of the signal between the nerves and muscle. Depending on individual circumstances, it may be necessary to give drugs that will suppress the immune system to stop it attacking the receptors.
What is the prognosis?
In mild cases prognosis is generally good and a complete recovery can be achieved. Repeated blood tests to measure anti-AChR antibody levels will be required. In more severe cases (especially if the problems swallowing lead to severe pneumonia) the prognosis is quite guarded. The earlier the diagnosis is made and treatment is started the higher is the chance of a successful outcome. Some patients will go into remission over 6 months.
Meningoencephalitis of unknown aetiology (MUA)
What is MUA and what are the causes?
Meningoencephalitis of unknown aetiology (MUA) is the umbrella term for multiple diseases including granulomatous meningoencephalitis (GME), necrotising meningoencephalitis (NME) and necrotising leukoencephalitis (NLE). These different types of inflammation can only be distinguished by brain tissue biopsy or post-mortem, hence the normal descriptive diagnosis of meningoencephalitis of unknown aetiology (MUA).
The exact cause of MUA is unknown, however it is thought to be an immune mediated disease where the dogs own immune system attacks its brain tissue (and sometimes the spinal cord). There is likely a genetic factor and a ‘triggering’ environmental factor that leads to dogs developing this condition.
Which pets typically get MUA?
Dogs of any age and breed can develop MUA, however we typically consider young-middle aged toy and small breeds to be more likely to develop this condition.
It is not contagious and therefore it is not spread from dog to dog.
What are the signs of MUA?
The signs seen from MUA can be very variable, and are dependent on the part of the brain and meninges that is inflamed. Signs that may be seen include seizures, changes in behaviour, reluctance to move the neck and changes in gait.
How is MUA diagnosed?
The diagnosis of MUA cannot be based solely on the clinical and/or neurological signs as other neurological conditions (e.g. tumours) can potentially cause similar signs.
Diagnosis is usually based on a combination of history, neurological examination, imaging (such as MRI) and cerebrospinal fluid (CSF) analysis. We will usually take bloods as well to rule out any other causes of inflammation such as infections.
What treatment options are available?
The mainstay of treatment for MUA is immunosuppression with high doses of steroids (dexamethasone, prednisolone). Steroids have multiple side effects including weight gain, polyphagia, polydipsia, panting and muscle wastage. It is our goal to reduce the steroid therapy to as low as dose as possible to ensure that the MUA is controlled in remission. Many cases need lifetime treatment and relapse frequently occurs.
More recent evidence has shown that a combination of both steroids and a chemotherapeutic agent called Cytarabine may improve prognosis in some cases. Cytarabine is given by infusion over 8 hours. Each case is treated and managed as an individual.
What is the prognosis?
Unfortunately, the prognosis for MUA is highly variable: approximately 25% of dogs will die or be euthanised in the week following diagnosis. Others will enter full or partial remission from the disease and maintain a normal or very good quality of life for many months or years. Prognosis is often based on initial response to treatment.
Steroid responsive meningitis and arteritis (SRMA)
What is SRMA?
Steroid responsive meningitis-arteritis (SRMA) in dogs is an ‘immune-mediated’ or ‘auto-immune’ condition where inflammation occurs in the blood vessels in the outer covering of the nervous system (the meninges). The condition most likely occurs because the dog’s immune system produces antibodies against a normal body protein causing inflammation. In SRMA this is a protein expressed by the walls of blood vessels in the meninges.
Despite extensive research we are not able to say why some dogs develop SRMA. Several studies have been performed looking at possible triggers including demographic, social, environmental, and medical factors. Breed was the only significant predisposing factor (see breeds listed below). Of particular importance, one study specifically evaluated risk associated with vaccination and identified no correlation between type or timing of vaccination and risk of developing SRMA. It is most likely that a complex interaction of genetics and the dog’s environment contribute to developing the condition.
There is no infection with this condition and the condition is therefore not contagious.
Which pets experience SRMA?
SRMA is diagnosed most commonly in dogs between 6-18 months of age, although dogs as young as 3 months and as old as 9 years have been reported with it. SRMA can occur in any breed but is most common in Beagles, Border Collies, Boxers, Bernese Mountain Dogs, Jack Russell Terriers, Weimaraners and Whippets.
What are the signs of SRMA?
Two different forms of SRMA may occur: acute and chronic. The main clinical signs of the acute form of SRMA are spinal pain, a stiff gait, reluctance to move the neck, a hunched back and often a fever. The pain is often worse in the neck but can also be present to some extent throughout the spine. In all but the most severe cases the neurological examination will be normal. Most dogs will have a reduced appetite and be reluctant to exercise. Inflammation can affect other parts of the body including the joints which can cause a stiff and stilted gait. Some dogs with SRMA can have inflammation of other inner body surfaces, like the covering of the heart (potentially causing abnormal heart rhythm), lungs and abdominal contents, causing the development of some fluid and episodes of diarrhoea and vomiting.
How is SRMA diagnosed?
The diagnosis of SRMA is made by taking a thorough history of your dog’s clinical signs followed by a physical and neurological examination. A diagnosis is normally made on the basis of firstly excluding other causes of spinal pain (like bone, muscle or soft tissue infections, immune-mediated joint disease, or trauma to the neck) with blood tests and either X-rays or advanced imaging such as MRI or CT. A spinal fluid sample is collected from the neck or lower back (or both) in a sterile manner under general anaesthesia. The cells in the spinal tap are examined for large numbers of a specific type of inflammatory cell which allows us to make a diagnosis.
Measurement of inflammatory markers in the spinal fluid and blood such as C-reactive protein (CRP) IgA levels have been used to aid in the diagnosis of SRMA. Assessment of these inflammatory markers can be useful in distinguishing SRMA from other diseases that can cause similar clinical signs. Serum CRP in particular can also be useful in monitoring for treatment efficacy and relapse.
What treatment options are available?
The main treatment for SRMA is suppression of the immune system with drugs, particularly high doses of corticosteroids like prednisolone. The administration of high doses of steroids by injection or orally usually results in significant and rapid improvement or resolution of the clinical signs. The steroid dose is then reduced slowly over the course of several months until the stimulus for the immune system has gone. Side effects are often seen with steroid use include increased thirst and hunger, increased urination and weight gain. Dogs can be more reluctant to exercise, pant more and are at increased risk of infections (respiratory, urinary). Occasionally additional medications are required to aid suppression of the immune system, or to allow us to reduce the steroid dose without fear of relapse. All medications can be given to your pet at home.
What is the prognosis?
Overall, the prognosis for SRMA is fair to good. The majority of dogs (80-100%) respond to initial treatment with immunosuppressive corticosteroids. While the initial response rate is excellent approximately one third of dogs will suffer at least one relapse during their lifetime. Some dogs will experience multiple relapses despite appropriate treatment. Relapse typically occur when steroid treatment comes to an end with clinical signs recurring a median of 8-28 days following discontinuation of treatment. There are also reports of dogs relapsing up to 1.5 – 2 years after discontinuation of treatment. Fortunately, a large proportion of dogs that suffer a relapse will positively respond to re-initiation of immunosuppressive therapy. Dogs that suffer a relapse may be successfully weaned off of treatment after long-term therapy; however, some will require a degree of life-long therapy to control their disease.

